What is Trauma-Informed?
The trauma-informed movement is picking up speed these days. But, do you know what it really means? In this piece, I offer a history of the trauma-informed movement, an outline of the trauma-informed framework, and a distinction between trauma-informed and trauma-specific care. This article is a follow up to my article entitled What is Trauma? If you haven’t read it, you might want to start there.
History of the Trauma-Informed Movement
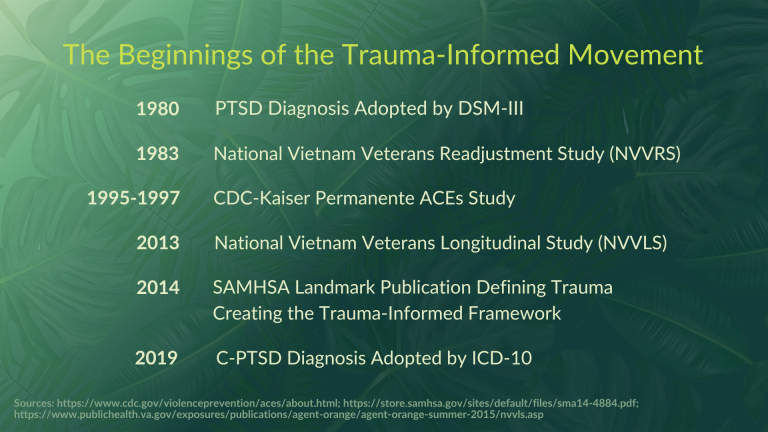
1980 - Post-Traumatic Stress Disorder (PTSD) is Included in the DSM-III
After the Vietnam War, the Veteran’s Administration was faced with the undeniable evidence that massive numbers of vets returning from overseas were unable to re-enter into their home lives. They were experiencing disruptions in sleep, cognition, and emotional regulation related to the re-experiencing of traumatic wartime events. It took a decade of advocacy for this experience to be named Post-Traumatic Stress Disorder (PTSD) and adopted into the third Diagnostic and Statistical Manual (DSM-III). This diagnosis paved the way for funding for research and treatment of this debilitating condition. See the What is TRAUMA? post for a full description of the diagnosis.
1983 - National Vietnam Veterans Readjustment Study (NVVRS)
In 1983, Congress asked the VA to conduct a study to determine the prevalence of PTSD in Vietnam veterans. It was found that up to 15% of all veterans had PTSD.
1995-1997 - CDC/Kaiser Permanente Joint Study on Adverse Childhood Experiences (ACEs)
In the early 90s, Kaiser had a massive weight loss initiative that was largely very successful. They found that NEARLY ALL of the participants who successfully lost weight and then subsequently regained the lost weight shared some troubling experiences. This discovery inspired the ACEs study which examined how patient history correlated to a variety of negative outcomes (health, health risk behaviors, mental health, and social). The findings were alarming. The more ACEs a person experiences, the risk of negative outcomes is compounded. The ACEs study is so significant because it expands the concept of trauma to include conditions that some of us think of as more or less normal. Chronic stress resulting from these conditions wreak havoc on our developing nervous system and sense of self.
Here are some ACEs statistics:
- 1 in 6 adults experience 4 or more types of ACEs
- At least 5 of the 10 leading causes of death are associated with ACEs
- 61% of adults had at least one ACE and 16 % had four or more types of ACEs
- Females and racial/ethnic minority groups were at greater risk for experiencing 4 or more ACEs
- Individuals with ACE scores of 4 or more were 12 times more likely to have attempted suicide
- People with ACE scores of 4 or more were 7 times more likely to be alcoholic,
- People with ACE scores of 4 or more were 10 times more likely to be have injected street drugs
- People with ACE scores of 6 and higher have an almost 20‐year shortening of lifespan.
For more on the ten Adverse Childhood Experiences and associated outcomes, see the What is TRAUMA? post.
2013 - National Vietnam Veterans Longitudinal Study (NVVLS)
Congress requested a follow up to the NVVRS to examine the long-term health and mental health of Vietnam Veterans. While most veterans were continue healthy lives, the outcomes for those who had had PTSD in 1987 were, again, alarming.
Here are just a few of the findings:
- 11% of male and 7% of female theater vest (as opposed to non-theater Vietnam era vets) still suffered from PTSD.
- 37% of theater vets with PTSD met criteria for Major Depression as compared with less than 1% of vets with no PTSD.
- Male theater vets with PTSD were twice as likely to have died
- Two thirds of of Veterans with current warzone related PTSD discussed behavior health or substance abuse issues with providers.
2014 - SAMHSAs Landmark Publication Defining Trauma and Creating the Trauma-Informed Framework
SAMHSA is the Substance Abuse and Mental Health Services Administration and it is a division of the U.S. Department of Health and Human Services. In this publication, they asserted that trauma is, “widespread, harmful and costly public health problem.” In addition to defining trauma, they developed a framework for delivery of trauma related services in public institutions. This framework consisted of the Four Rs, Six Guiding Principles, and the 10 Domains for Implementation. See the section below for a full explanation of the framework
What is the Trauma-Informed Framework?
The Four R's of Trauma-Informed Care
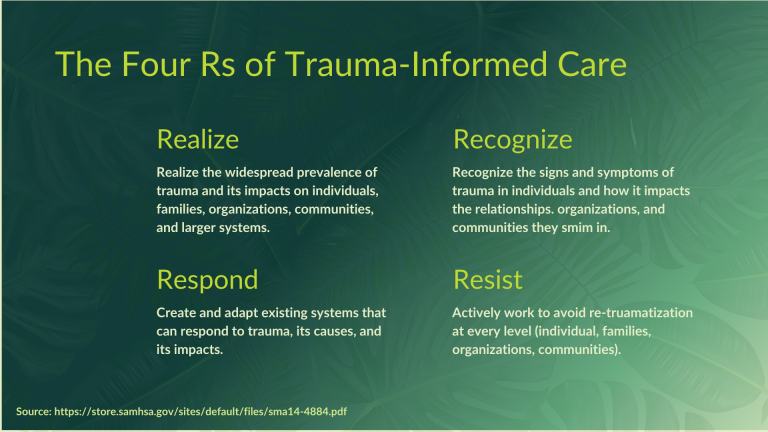
Realize
We must realize the widespread prevalence of trauma and its impacts on individuals, families, organizations, communities, and larger systems.
Recognize
We must recognize the signs and symptoms of truama in indviduals and how it impacts the relationships, organizations, and communities in which they swim.
Respond
We must adapt existing systems and create new ones that can respond to trauma, its causes, and its impacts. See the 10 Domains of Implementation.
Resist
We must actively work to avoid re-traumatization at every level (individual, families, organizations and communities).
Six Guiding Principles of Trauma-Informed Care
Safety
Recipients and providers of care do so in an environment of physical and psychological safety.
Trustworthiness and Transparency
Operations and decisions are conducted with transparency and the goal of building and maintaining trust among staff, clients, and family members of those receiving services. People do what they say they will.
Peer Support
Utilize the support of peers to build trust and foster healing.
Collaboration and Mutuality
There is recognition that healing happens in relationships and in the meaningful sharing of power and decision-making. The organization recognizes that everyone has a role to play in a trauma-informed approach. One does not have to be a therapist to be therapeutic.
Empowerment, Voice, and Choice
Aim to strengthen the staff, client, and family members’s experience of choice and recognize that every person’s experience is unique and requires an individualized approach. This builds on what clients, staff, and communities have to offer, rather than responding to perceived deficits.
Cultural, Historical, and Gender Issues
Actively move past cultural stereotypes and biases. Offer culturally responsive services. Leverage the healing value of traditional cultural connections. Recognize and address historical trauma
10 Domains for Implementing Trauma-Informed Care
The SAMHSA framework grew out of an awareness that the systems and organizations that exist to help folks who have experienced trauma, are also re-traumatizing. These are the 10 domains in organizations to which we must apply the Four Rs and the Six Guiding Principles.
Governance and Leadership
Are leadership and governance accessible to constituents? Are leaders accounting for the experiences of marginalized and traumatized people? Are leaders representative of those they serve?
Physical Environment
Is the physical environment conducive to a Rest and Digest state of being for both recipients and providers of services? This can include ease of access to restrooms and quiet spaces, appropriate temperatures, places to sit, information/signage that is accessible to all of those providing and seeking services. Is the physical space free of violence and intimidation of any kind?
Engagement and Involvement
Are the people who seek services engaged and involved in shaping the delivery of services?
Cross Sector Collaboration
Is our organization informed by what is known by our partners? Would a cross sector collaboration make service delivery more seamless and accessible.
Screening, Assessment, and Treatment Services
This applies mostly to health/mental health services. Does the way that we screen, assess, and treat support overall healing and well-being. Is the process itself re-traumatizing?
Progress Monitoring and Quality Assurance
Have we succeeded in creating an environment of safety and offered services and resources for those who have experienced trauma? Are we asking ourselves, how we are doing? How satisfied are people who have sought and received services?
Training and Workforce Development
How are employees and leaders at every level supported to embody and enact a healing environment and relationships/interactions. Are trainings and workforce development themselves re-traumatizing? Are we doing this to fulfill a mandate, or do we care about how WE impact those we serve? Are we consulting marginalized and survivors of trauma when we design trainings and development?
Evaluation
In the process of evaluating employee and leader performance, do we ask, is trauma begetting trauma? Have our employees and leaders had access to the resources for healing and done the work? Are our triggers and dissatisfaction leaking out onto those we serve?
Financing
Is there funding in place for enacting polices that support healing and recovery?
Policy
Are there polices in place that dictate how to evaluate, finance, govern, and provide services that do not re-traumatize and, in fact serve to support healing and recovery? Have survivors been involved in developing these policies?
Trauma-Informed vs. Trauma Specific
I see a lot of confusion around this distinction. Trauma-informed is everything described in the section above and offers a framework for providing services without doing harm. Some of those services may be trauma-specific. You can absolutely be trauma-informed without being trauma-specific. I offer this as an invitation to honor your scope of practice and expertise when providing services.
Trauma-Informed
- See above description of the Trauma-Informed Framework (Four Rs, Six Guiding Priciples, and 10 Domains for Implementation.
- An approach to service delivery.
- Emphasizes physical, psychological and emotioanl safety for both providers and recipients of care.
- Creates opportunities for survivors to rebuild a sense of agency and empowerment
- Anticipates and avoids institutional processes and individual practices that are likely to re-traumatize individuals with a history of trauma.
- Asserts that survivors should be part of the process by which these policies and practices are created
Trauma-Specific
- Services specific to the treatment and/or healing of trauma
- Involves clinical training to track and work directly with the nervous system and psychodynamic processes.
- Addresses (directly or indirectly) the traumatic event/s in order to renegotiate how the experience is held in the body, memory and identity.
Let's do this...
The great news is that the trauma-informed movement is growing fast! If you are a coach or practitioner who would like to join the groundswell, let’s have a chat. I offer a Trauma-Informed Practice Groups with cohorts starting quarterly. Join me in bringing this awareness to the services you provide.
SHARE THIS PAGE…