What Is Trauma?
We throw the term around, but what does it really mean? This is an introduction to trauma and its various forms.
Definitions of trauma vary widely across domains of study. These definitions are synthesized from several dictionary listings and mental health resources that exemplify the most current understanding in the identification and treatment of trauma
trauma /ˈtrômə/
1. an event or condition that is experienced as distressing or disturbing and overwhelms an individual’s nervous system.
2. the lasting negative impacts of traumatic experiences on mental, emotional and physical well-being.
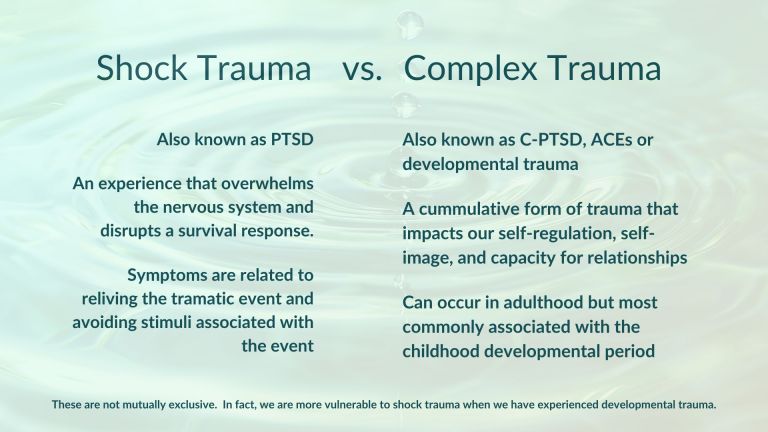
Types of Trauma - Shock Trauma vs. Complex Trauma
These two forms of trauma are not mutually exclusive. In fact, complex trauma makes us more vulnerable to shock trauma. AND, shock trauma may reactivate latent complex trauma that was not problematic before the event.
Shock Trauma (PTSD)
Shock trauma, also known as Post-Traumatic Stress Disorder (PTSD), results from an event that overwhelms a person’s ability to react and complete a survival response. These are events that are perceived as life-threatening (to self or other). The disruption of a threat response mainly involves the brain stem. Treatments therefore, are concerned with reengaging and completing autonomic (non-voluntary) reactions that are outside of the direct control of the prefrontal cortex.
Examples of events that can lead to shock trauma (PTSD)
- Natural Disaster
- Combat/War
- Witness or Victim of Violence
- Car Accident
- Traumatic Fall
- Medical Emergencies
- Unexpected Loss (especially of a loved one)
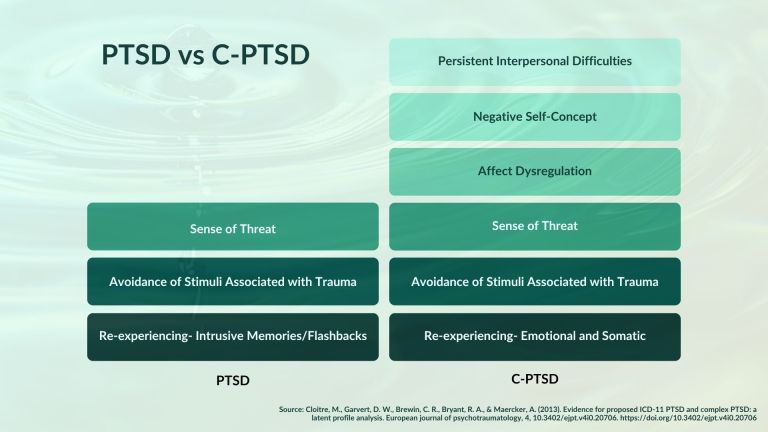
Signs and Symptoms of Shock Trauma (PTSD)
- Re-experiencing: Intrusive Memories/Flashbacks
- Hypervigilance to Stimuli Related to Truamatic Event
- Avoidance of Stimuli Associated with Traumatic Event
- Sense of Threat
Complex Trauma (C-PTSD)
Complex trauma is by definition more complex. In complex trauma, the traumatic condition is ongoing or pervasive in nature. Even more complex is when these conditions are the backdrop to our childhood and adolescent development. Our entire identity, nervous system, and way of relating to the world are formed around these traumatic conditions. In NARM we call these conditions that fail to meet our developmental needs, environmental failures. Neccessarily, the threat is to our sense of self. That said, the threat may also have been physical, making symptoms of PTSD engrained in who we take ourselves to be.
Examples of events that can lead to complex trauma (C-PTSD)
- Adverse Childhood Experiences (ACEs see below)
- Bullying
- Living in Wartime
- Systemic Oppression or Marginalization for Any Reason
- Life-threatening or Chronic Illness
- Separation from Caregiver, Adoption and Foster Care (Attachment Trauma)
- Violence in the Community
Signs and Symptoms of Complex Trauma (C-PTSD)
- Re-experiencing: Emotional and Somatic Flashbacks
- Avoidance of Stimuli Associated with Trauma
- Sense of Threat
- Emotional Dysregulation
- Negative Self-Concept/Low Self-Esteem
- Disrupted Capacity for Relationships
Adverse Childhood Experiences (ACEs)
The Adverse Childhood Experiences (ACEs) study was conducted jointly by the CDC and Kaiser between 1995 and 1997. By analyzing mountains of patient data and conducting interviews, they discovered the correlation between ACEs and some alarmingly negative outcomes in all areas of life including physical, mental, and social health. Even more significant is that these experiences are cumulative or compounded. The more of these that we have experienced, the worse the outcomes.
What are ACEs?
The ACEs study identified ten conditions or experiences that had the strongest correlation to negative outcomes. I’ll add here that all ACEs are examples of developmental trauma or attachment trauma. All trauma that happens in childhood, even if it is a shock trauma at the time, is developmental trauma because it happened during the developmental period. When the nervous system and sense of self develops around (adapts to) these conditions, the impacts are systemic and pervasive with no reference point of wellness before the trauma.
The 10 ACEs
- Physical Abuse
- Sexual Abuse
- Emotional Abuse
- Physical Neglect
- Emotional Neglect
- Mental Illness in the Household
- Violence in the Household (Specifically against Mother)
- Incarcerated Family Memebers
- Alcoholism or Substance Abuse
- Parental Divorce
Outcomes Associated with Adverse Childhood Experiences
Here are the outcomes the Kaiser-CDC ACEs study linked to these detrimental conditions (in NARM, environmental failures). The outcomes that the ACEs study failed to mention are much more subjective and will be addressed in the next section (Impacts of Developmental Trauma).
Chronic Health Conditions
- Coronary Heart Disease
- Stroke
- Asthma
- Cancer
- Kidney Disease
- Obesity
- Chronic Obstructive Pulmonary Disease (COPD)
Health Risk Behaviors
- Smoking
- Excessive Alcohol Use
- Substance Misuse
- Physical Inactivity
- Sexual Risk Behaviors
- Suicidal Thoughts/Behaviors
Social Outcomes
- Lack of Health Insurance
- Unemployment
- Less than High School Diploma/Equivalent
Mental Health Outcomes
- Depression
- Substance/Alcohol Use Disorder
Impacts of Developmental Trauma
Again, the outcomes of ACEs are cumulative. In the graphic below, we can see how ACEs fit into the broader social and historical context. ACEs arise from generational and historical trauma which then shape the social and local conditions of the environment. In other words, it didn’t start with you…or even your parents.
The Mechanism by Which ACEs Influence Health and Well-Being Throughout the Lifespan
Again, the outcomes of ACEs are cumulative. In the graphic below, we can see how ACEs fit into the broader social and historical context. ACEs arise from generational and historical trauma which then impact and shape the social and local conditions of the environment. In other words, it didn’t start with you…or even your parents.
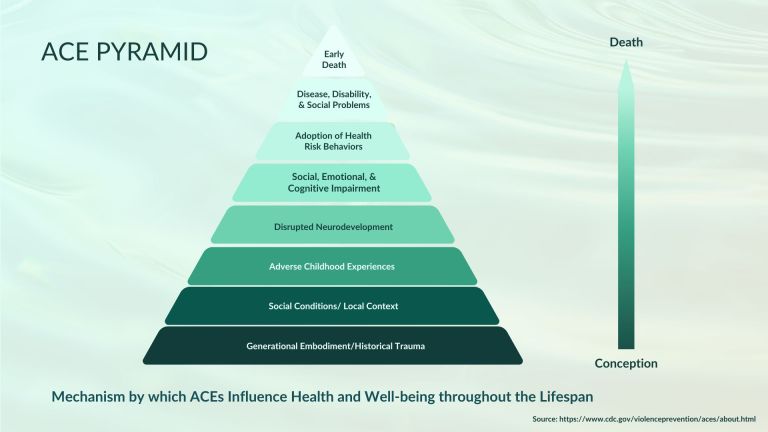
The ACEs Pyramid (from the bottom up)
- Generational Embodiment/Historical Trauma
- Social Conditions/Local Context
- Adverse Childhood Experiences (ACEs)
- Disrupted Neurodevelpment
- Social, Emotional, & Cognitive Impairment
- Adoption of Health Risk Behaviors
- Disease, Disability, & Social Problems
- Early Death
The ACEs Pyramid Statistics
- 1 in 6 adults experience 4 or more types of ACEs
- At least 5 of the 10 leading causes of death are associated with ACEs
- 61% of adults had at least one ACE and 16 % had four or more types of ACEs
- Females and racial/ethnic minority groups were at greater risk for experiencing 4 or more ACEs
- Individuals with ACE scores of 4 or more were 12 times more likely to have attempted suicide
- People with ACE scores of 4 or more were 7 times more likely to be alcoholic,
- People with ACE scores of 4 or more were 10 times more likely to be have injected street drugs
- People with ACE scores of 6 and higher have an almost 20‐year shortening of lifespan.
What Happens in the Nervous System
The graphic below is one I adapted to include/emphasize the nervous system impacts of developmental trauma. It is adapted from a classic polyvagal chart that focused on shock trauma responses and language.

POLYVAGAL THEORY
In an attempt to distill a very complex topic, I’ll limit this section to the parts of the autonomic nervous system and how they might be distorted by trauma. When an actual or perceived threat occurs, the “normal”, or “healthy” wave of sympathetic arousal is disrupted. If we are able to return to the normal wave after a threat, then there is no lasting trauma. In complex trauma, we may experience very complex patterns and combinations of these responses.
Sympathetic
This what we know of as FIGHT or FLIGHT. I’ve added FAWN here as another option that happens in a state of arousal as a result of complex trauma. Sympathetic arousal is associated with increased heart rate, decreased digestion and immune function, and dilated pupils. In other words, all energy expenditure in the body is rallied for action to either avoid or protect from threat. The statements that represents this state, depending on the intensity of the arousal are “I CAN,” or “I MUST.”
Parasympathetic
The parasympathetic nervous system has two branches that are mediated by the vagus nerve and serve very different functions.
Ventral Vagal
Also know as REST and DIGEST or the SOCIAL ENGAGEMENT SYSTEM, the ventral (frontal) branch of the vagus nerve is ideally where we spend most of our time. It is characterized by a calm alertness. Digestion and immune function are at their optimum capacity. Energy expenditure supports our inclination toward exploration, curiosity and connection in the present moment. The statement that represents the ventral vagal state is, “I MAY.” As in, if I want to.
Dorsal Vagal
The dorsal (back) branch of the vagus nerve provides the FREEZE response. Freeze is what happens when we have (or believe we have) no other option. It is a total system shut down and energy conservation. The barest minimum of energy is expended to maintain life support. It is meant to be very time-limited and is, in itself, life-threatening when it continues too long. In the world of critters, we know this as “playing dead” but in humans, it is more commonly associated with numbness, depression, and dissociation. The statement that represents the dorsal vagal state is, “I CAN’T.”
Attachment Theory
Attachment theory, developed by John Bowlby, posits that the quality of our attachment with our primary caregiver(s) has significant and lasting impacts on how we relate to ourselves, other people, and the world. The attachment serves shifting purposes as a child moves through developmental phases. Failures or disruptions to meeting the attachment needs at various developmental stages give rise to what some call attachment styles. In NARM, we call these Adaptive Survival Styles. Each of these styles has tendencies toward certain patterns of arousal/shutdown or tension/collapse.
Commonly Missed Signs of Developmental Trauma
The severity and pervasiveness of developmental/attachment trauma exists on a continuum from mild disruption of development, to profound cognitive, affective, and relational deficiencies. Listed below are some common challenges that we might not think of impacts of trauma. It is a rare one among us who escapes childhood having all of their developmental needs perfectly met.

- Overwhelm
- Inner Critic
- Limiting Beliefs
- Fear of Failure
- Perfectionism
- Conflict Avoidance
- Imposter Syndrome
- Difficulty Speaking Up
- People Pleasing
- High Sensitivity to Anger in Self and Others
- Reactivity to Feedback
- Difficulty Acknowledging and Advocating for Needs
- Difficulty Saying "No" or Setting Boundaries
- Health Problems Related to Chronic Stress or Inflammation
- Challenges with Empathy or Perspective Taking
- Chronic Resentment, Passive Aggression, or Martyring
- Difficulty Delegating or Trusting a Team
- Disorganization and Time Management Issues
In Closing...
Thanks for sticking with me. I hope this (not so brief) introduction to trauma has been clarifying. In the future, this material will be part of a course on trauma-informed coaching. If you are seeking support or are interested in learning more about healing and trauma, schedule a complementary consultation.
Join the community
SHARE THIS PAGE…